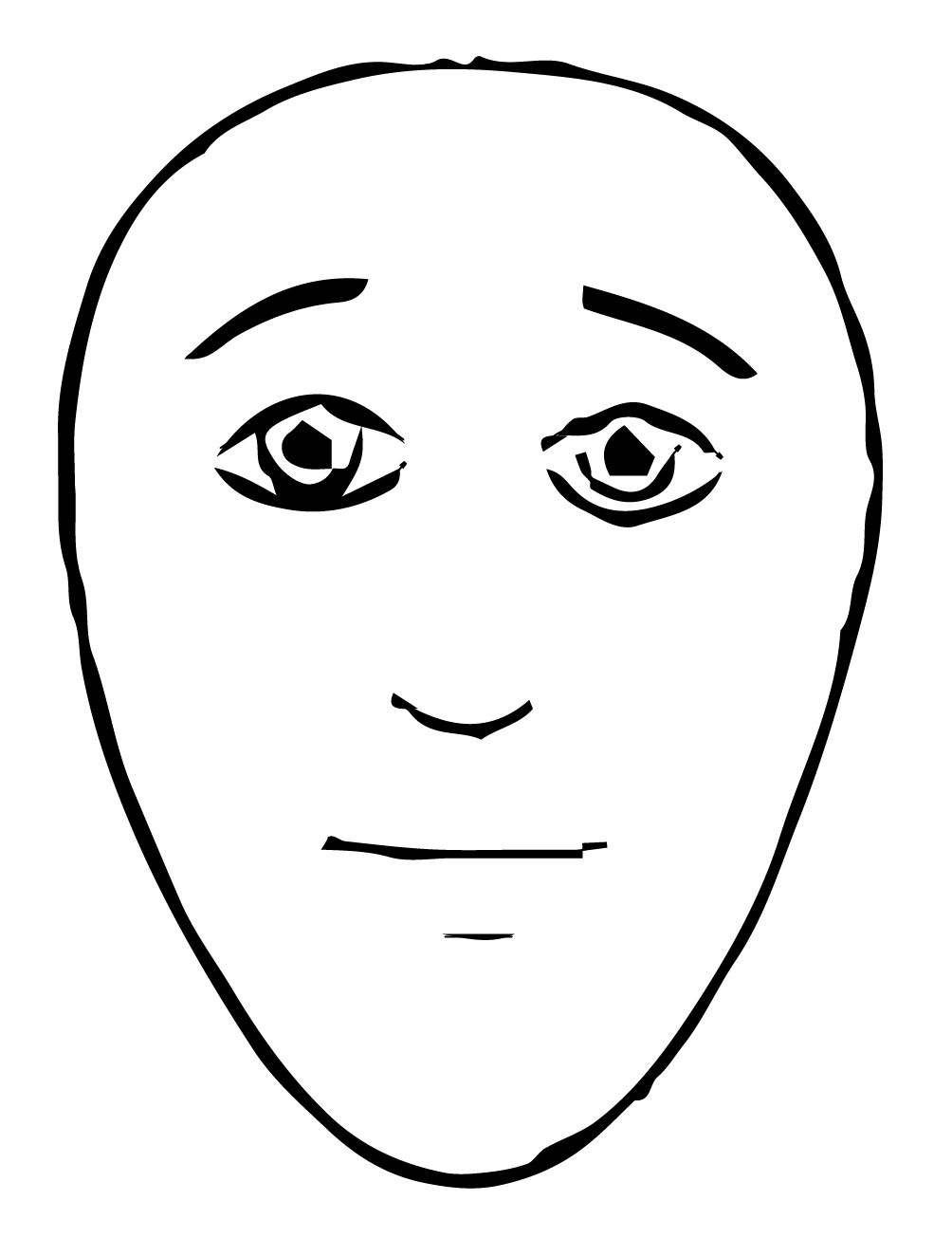
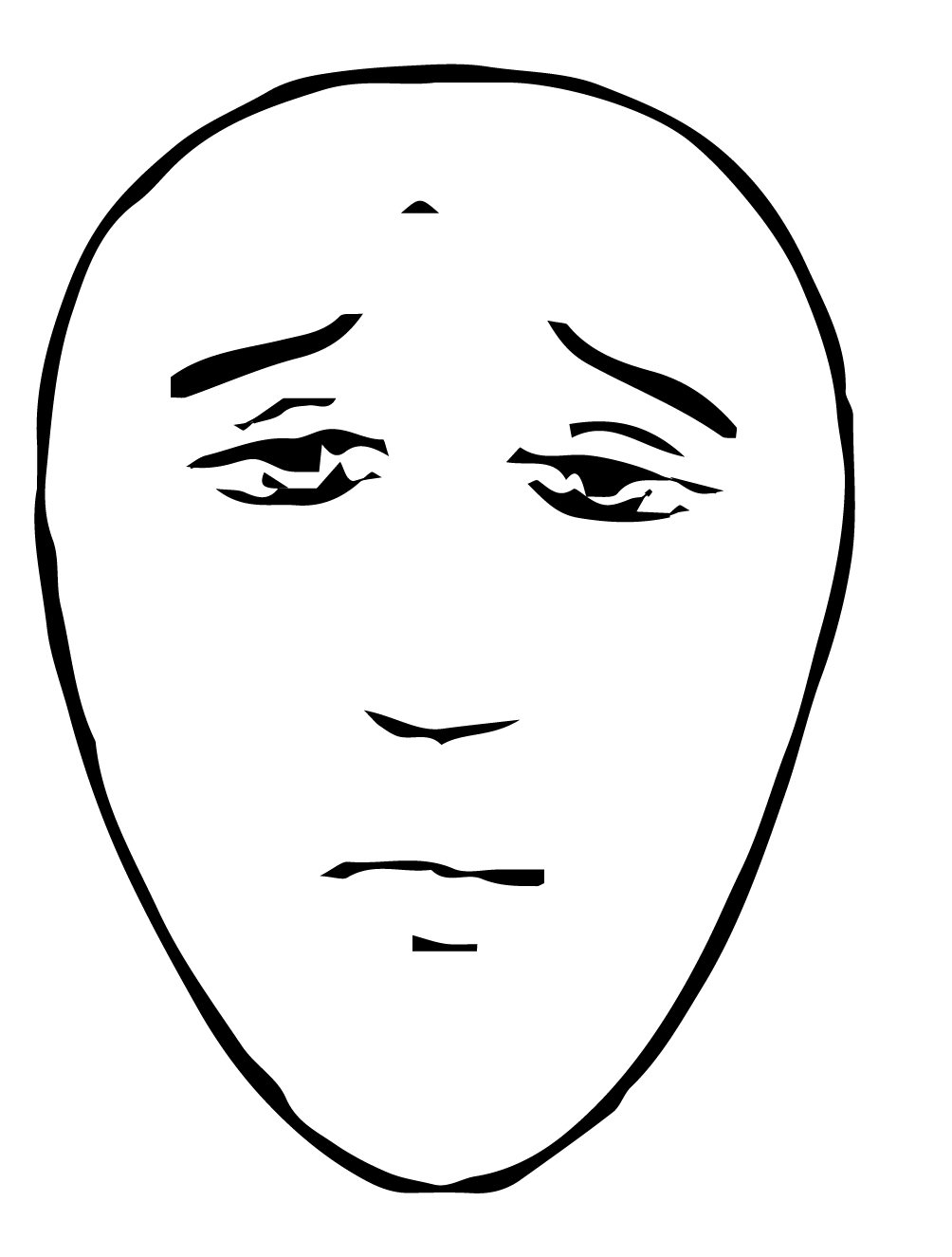
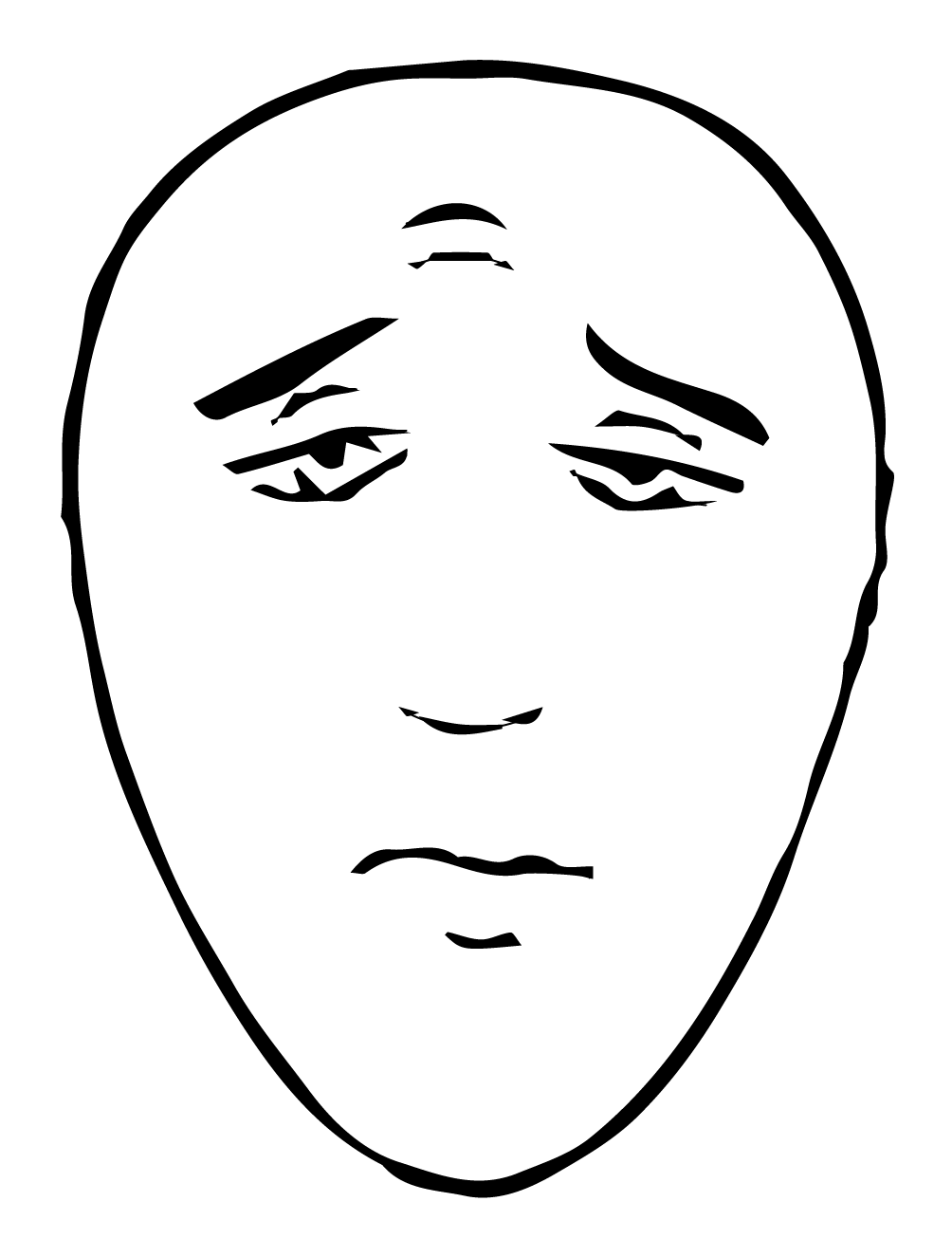
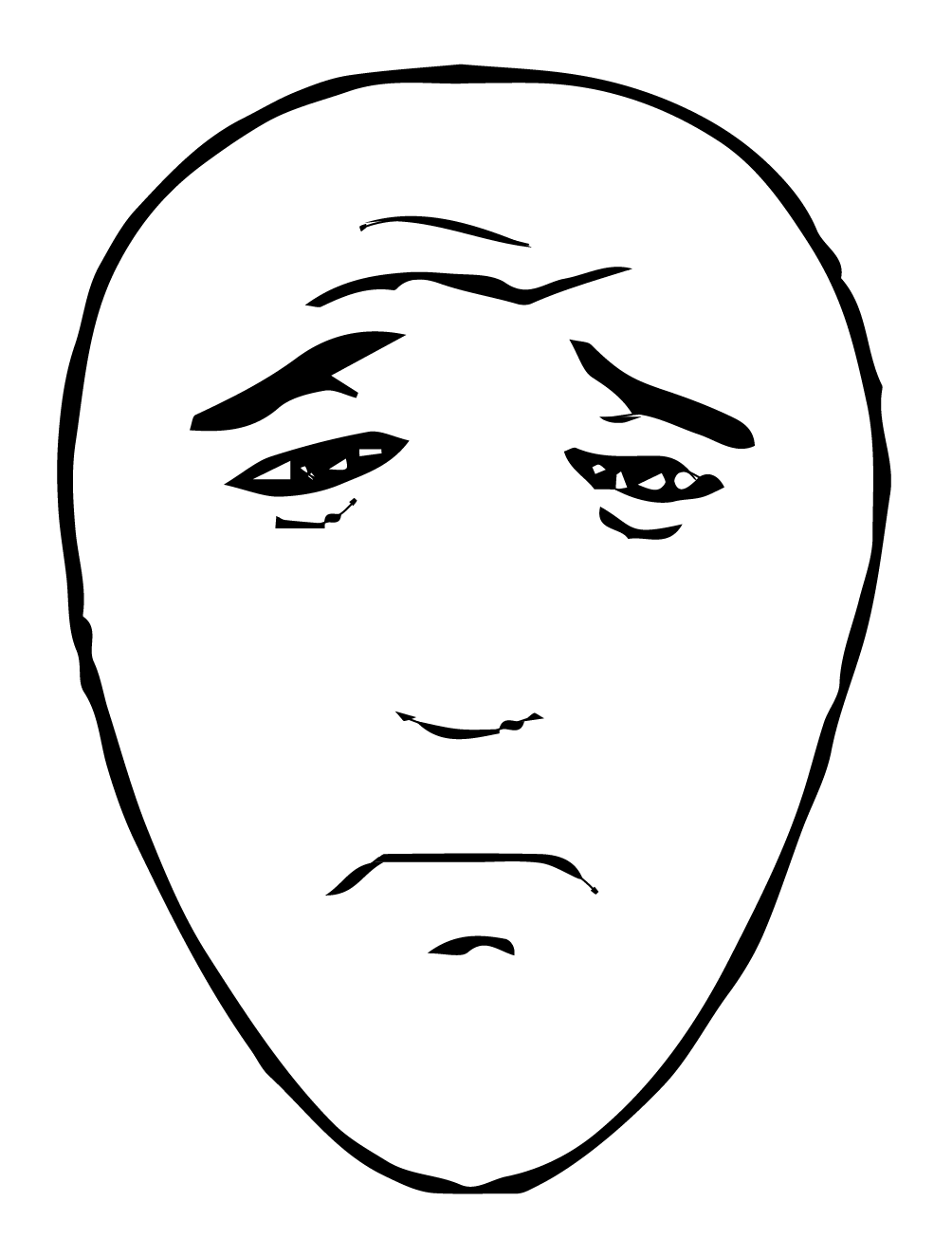
| Rating System | The Faces Pain Scale uses drawn faces to represent pain levels on a scale of 0 to 5. |
|---|---|
| Common Use | Most commonly used with children aged 3+, may also be used for adults with cognitive impairments. |
| Instructions | This scale is intended to measure how the patient feel inside, not how their face looks. The pain scale is shown to the patient with these instructions: “These faces show how much something can hurt. This face [point to face above number “0”] shows no pain. The faces show more and more pain up to this one [point to the face above number “5”] – it shows very much pain. Point to the face that shows how much you hurt [right now].” |
| 0 | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
 |
 |
 |
 |
 |
 |
Source: Hicks, C. L., von Baeyer, C. L., Spafford, P. A., van Korlaar, I., & Goodenough, B. (2001). The Faces Pain Scale – Revised: Toward a common metric in pediatric pain measurement. Pain, 93, 173-83.
| Rating System |
|---|
| The Faces Pain Scale uses drawn faces to represent pain levels on a scale of 0 to 5. |
| Common Use |
| Most commonly used with children aged 3+, may also be used for adults with cognitive impairments |
| Instructions |
| This scale is intended to measure how the patient feel inside, not how their face looks. The pain scale is shown to the patient with these instructions: “These faces show how much something can hurt. This face [point to face above number “0”] shows no pain. The faces show more and more pain up to this one [point to the face above number “5”] – it shows very much pain. Point to the face that shows how much you hurt [right now].” |
| Number | Visual |
|---|---|
| 0 | |
| 1 | |
| 2 | |
| 3 | |
| 4 | |
| 5 | |
Source: Hicks, C. L., von Baeyer, C. L., Spafford, P. A., van Korlaar, I., & Goodenough, B. (2001). The Faces Pain Scale – Revised: Toward a common metric in pediatric pain measurement. Pain, 93, 173-83.